In just a few weeks, I'll be flying to Seattle, WA to participate in and enjoy the AHCAE's national conference. The AHCAE's focus is how auditing and education come together to help providers and payers ensure documentation, coding, and billing are compliantly optimized. In that vein, I thought this article might be best used to highlight some elements of auditing that are beginning to gain steam and are sometimes overlooked or at best, shuffled to the bottom of the concern stack.
Take a look at this HPI (history of present illness) - any concerns?
Mouse Over Image to enlarge
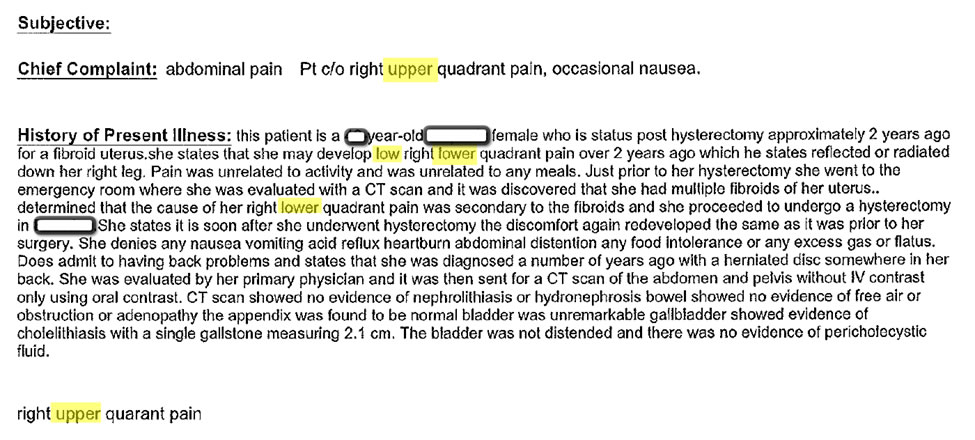
Notice anything wrong here? Want this projected on a courtroom wall for the
world to see? I can just hear the opposing counsel - "Doctor, do you know where
this patient's pain actually was? What were you treating?" Yikes. Just know
that all the warts in the record could end up just that way - so make sure there
are as few warts as possible - right?
How about another:
Mouse Over Image to enlarge
Mouse Over Image to enlarge
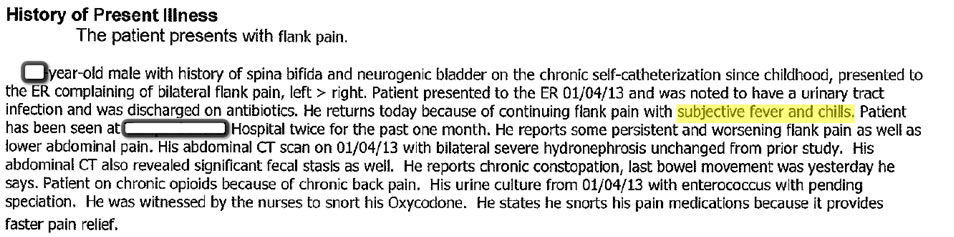
Okay, provider, did the patient have fever and chills or not and how about constipation,
abdominal pain and back pain? How are we to trust this documentation when there's
a conflict? Is the ROS truly updated on this date by the provider or a pull
forward? Another gotcha!
All this to say that what is in the documentation and what is in the templates
of our EHRs (e.g., what our defaults say) do matter. These are not only CPT
billing risks but also malpractice concerns. Have you checked to see if your
malpractice carrier has any criteria on documentation within an EHR? Will you
be covered by insurance should a case be presented? Do you even know what your
malpractice insurance would actually cover here? I'd say, check that out pretty
quick.
More importantly, what is the right documentation for this patient? Are we missing or confusing the patient's chart by 'fluffing the pillow' of documentation and letting templated defaults rule the day?
Another element to consider is for an EHR, the exact time an event was recorded and by whom is captured - that's subject to discovery. Did you review that diagnostic service before or after the patient had an adverse event? And, did you really even review it?
If your EHR pulls forward information (diagnostic data, historical information), are you confirming and updating the information during this encounter - if not, I should know that by reading the chart. If you are updating and confirming, I should also know that by reading the chart. You don't want old clinical information in a current chart if it conflicts with the current condition or has changed.
Do I know who did what in the encounter or is the bottom of the chart signed by two people (e.g., RN and MD)? I need to know who did what portions of the care and who documented each portion.
Take these steps to ensure you don't have malpractice issues due to the way you use your EHR:
- Remember, your record is the black box should something adverse happen to the patient.
- Make sure it's clear that those who access the EHR are the appropriate person to do so and that authentication is by the right person.
- Make doubly sure your providers know what the EHR contains (you'd be surprised at how many are unaware of what the printed record really contains) and how their interactions are reflected in the final record.
- Check to see if the documentation is an easy to follow record of events, work, outcomes, and treatments. Many times you have to read through the chart several times to try and glean what is really going on.
- Audit, audit, audit... make sure you are not caught in a predicament because of a poorly designed or used EHR.
Most providers do a good job of caregiving their patients and believe they are well documenting those efforts, but the process of using the EHR hides that good work - look for ways to improve documentation to truly reflect what occurs within the patient encounter.
Hope to see you at the AHCAE national conference in August or at an Intensive Chart Auditing Practicum to learn more!
Click here for more information on the 2014 AHCAE National Conference
Susan Garrison, CHCA, PCS, FCS, CHC, CPC, CCS-P, CPAR, CPC, CPC-H
Executive Director of Education, Association of Health Care Auditors and Educators
www.ahcae.org