There is little sleep going on in the healthcare world right now! From the front lines of the first responders to the back rooms full of coders and billers.
The whole world was thrown upside down in a matter of days! We now not only face the day-to-day personal living impacts of COVID-19, but as coders, billers, providers, and managers, we face the day-to-day changes of rules and coding associated with treating our patient base. These sweeping and continuous changes in guidance have many of us concerned for the backend impact post-PHE (Public Health Emergency). Of course, we understand it takes time to create and modify such changes, but will ill-defined guidance result in recoupments of the payments that are keeping our practices afloat at this time?
During this PHE, CMS and many commercial carriers have relaxed much of the existing telehealth guidance. Many of these new changes are even being changed within a day or two of release.
This has led to many questions, such as the following:
- Which code set should I use?
- Can I use audio only?
- What place of service (POS) should I use?
- Must I use a modifier?
- How can an exam be performed virtually?
- What role does time play in the virtual encounter?
- What about teaching physician services?
- How can I avoid getting laid off?
CMS has released an Interim Final Rule (IFR) for treating patients during this PHE, which can be found by a simple Google search for "CMS Interim Final Rule." As is normal, there is a comment period that ends at 5:00 pm on June 1, 2020. However, the Federal Register has noted the IFR as effective March 31, 2020 with applicability of March 1, 2020, meaning that services rendered since March 1, 2020 are subject to these relaxations and guidance. The publication is 221 pages in total, but most of these questions can be answered with merely a few pages of guidance. As we discuss each of the questions noted above, the source page number(s) will be provided for your reference.
Which code set should you use?
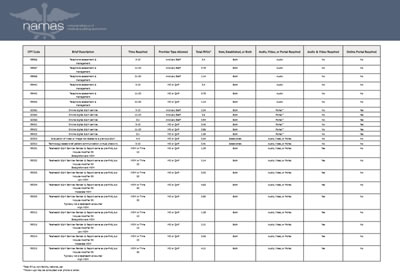
Below, you will find a chart that identifies the distinguishing facts of each recognized telehealth service.
Below, you will find a chart that identifies the distinguishing facts of each recognized telehealth service.
The brief overview is:
- CMS relaxed telehealth services.
- There are reimbursable services for audio communication only visits, as well as services that additionally require video.
- Direct supervision can be met via video communication.
- There are certain billing specific rules.
Patient Portal with no audio or video required (pages 53-54)
AMA implemented codes 99421-99423 for online communication between a MD/QHP with an established patient many years ago, but few payors reimbursed this service. CMS has recognized this during the PHE as a reimbursable service, and in addition, CMS has also created the code set G2061-G2063 that is reportable for online communications between ancillary staff and the patient.
Both sets of codes indicate that the code represents all time spent for the patient by the type of provider of the same group, i.e., cumulative time, in the past 7 days (see time per code in the chart below). While most portals have video and/or audio capability, the code set was originally created for encounters in which a patient would have, for example, an email encounter with the patient. This explains why it is not a requirement of the code set.
Both AMA and CMS code sets indicate the codes are reserved for established patients only, and for many telehealth services, CMS has relaxed this requirement as noted in the paragraph that follows the 99421-99423 and G2061-G2063 guidance for reporting:
In the context of the PHE for the COVID-19 pandemic, where communications with practitioners might mitigate the need for an in-person visit that could represent an exposure risk for vulnerable patients, we do not believe the limitation of these services to established patients is warranted. While some of the code descriptors refer to "established patient," during the PHE, CMS-1744-IFC 54 we are exercising enforcement discretion on an interim basis to relax enforcement of this aspect of the code descriptors. Specifically, we will not conduct review to consider whether those services were furnished to established patients.
Audio Only Services (pages 123-125)
Previously, CMS did not pay for 98966-98968 or 99441-99443 as non-face-to-face services were standardly a non-covered CMS service. During this time of PHE, CMS has relaxed this rule and allowed reimbursement for these services. The biggest difference between the two code sets is the rendering provider. In the chart below, you will note that 98966-98968 are rendered by Ancillary Staff while 99441-99443 are reserved for MD and QHP providers. Ancillary Staff are those individuals who provide services as part of the same Tax ID as the supervising provider, but CMS does not recognize them as billable individuals. The 99441-99443 telephone non-face-to-face service codes are to be used by MDs and QHPs (Nurse Practitioners, Physician Assistants, and Clinical Nurse Midwives).
Previously, CMS did not pay for 98966-98968 or 99441-99443 as non-face-to-face services were standardly a non-covered CMS service. During this time of PHE, CMS has relaxed this rule and allowed reimbursement for these services. The biggest difference between the two code sets is the rendering provider. In the chart below, you will note that 98966-98968 are rendered by Ancillary Staff while 99441-99443 are reserved for MD and QHP providers. Ancillary Staff are those individuals who provide services as part of the same Tax ID as the supervising provider, but CMS does not recognize them as billable individuals. The 99441-99443 telephone non-face-to-face service codes are to be used by MDs and QHPs (Nurse Practitioners, Physician Assistants, and Clinical Nurse Midwives).
The RVU allocation by CMS is consistent with AMA and noted in the chart below, but what is interesting is the RVU allocation for ancillary staff is the same as the code set for MD/QHP providers.
Audio & Video Services Required (pages 135-137)
In an effort to maintain continuity of patient care through this time of crisis with the easiest transition of billing/coding for these services, CMS has broadened the use of our outpatient/office E&M code category. What a relief this has provided to providers and their billing/coding teams! There are no new codes to figure out and no documentation modifications required. Rather, providers should continue to use the E&M service codes 99201-99215 as they would in their office, ensuring that documentation and medical necessity supports the level of service billed. The use of these standard office services has raised many questions about their virtual use.
Let's provide Q&A for the common concerns:
- Can new patient visits be performed?
Yes, this was an additional relaxation provided by CMS. - How is an exam performed virtually?
The provider can document visual exam findings just as they would in an exam room, as well as patient involvement. For example, the provider could document the patient respiratory effort (accessory muscle use or shortness of breath) and/or have the patient palpate their neck for swollen lymph nodes or palpate their abdomen for pain or guarding. - How is the documentation scored for leveling of the E&M service?
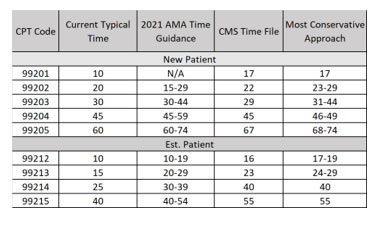
CMS has advised that we should base the level of service on the documented MDM or time, much like we will in 2021. The leveling difference between now during the PHE and the 2021 guidance is for now, we use the existing MDM rules and guidance. Therefore, during the PHE, we do not need to score the history or exam for telehealth services billed with the office/outpatient E&M code set. If, however, an encounter is billed based on time in lieu of MDM, we then use the 2021 definition of time. Therefore, the total time spent in conjunction with the encounter on that specific date of service may be combined toward the total time selected. Herein lies a concern, however. There is contradictory guidance in what total times we should use when selecting the level of service.
Within the IFR we find the following time guidance:
We note that currently, there are typical times associated with the office/outpatient E/Ms, and we are finalizing those times as what should be met for purposes of level selection. The typical times associated with the office/outpatient E/Ms are available as a public use file at: https://www.cms.gov/Medicare/Medicare-Fee-for-ServicePayment/PhysicianFeeSched/PFS-Federal-Regulation-Notices-Items/CMS-1715-F.
This policy CMS-1744-IFC 137 only applies to office/outpatient visits furnished via Medicare telehealth, and only during the PHE for the COVID-19 pandemic.
We note that currently, there are typical times associated with the office/outpatient E/Ms, and we are finalizing those times as what should be met for purposes of level selection. The typical times associated with the office/outpatient E/Ms are available as a public use file at: https://www.cms.gov/Medicare/Medicare-Fee-for-ServicePayment/PhysicianFeeSched/PFS-Federal-Regulation-Notices-Items/CMS-1715-F.
This policy CMS-1744-IFC 137 only applies to office/outpatient visits furnished via Medicare telehealth, and only during the PHE for the COVID-19 pandemic.
This creates confusion as there is certainly a discrepancy noted here. Here is a chart noting the differences in the AMA 2020 typical times, the times noted in the file provided by CMS, and the 2021 total times per AMA 2021 guidance (time range). Of note, it is recommended that each organization use the most conservative time for each level of service. The most conservative time would be the most time required to support that given level of service.
Place of service (POS) reporting (page 15)
This has been a point of confusion as CMS changed the original POS guidance. The IFR states that the encounter should be billed with the POS that the provider would have used had the encounter occurred outside of the PHE. Therefore, if your provider typically sees patients in an office setting utilizing POS 11, you could continue to use POS 11.
This has been a point of confusion as CMS changed the original POS guidance. The IFR states that the encounter should be billed with the POS that the provider would have used had the encounter occurred outside of the PHE. Therefore, if your provider typically sees patients in an office setting utilizing POS 11, you could continue to use POS 11.
Modifier Usage (page 15)
This guidance was also updated by CMS within the IFR. Therefore, modifier 95 should be appended to all services rendered as a telehealth type of service.
This guidance was also updated by CMS within the IFR. Therefore, modifier 95 should be appended to all services rendered as a telehealth type of service.
Modification of Direct Supervision (pages 56-57)
The IFR states that direct supervision, during the PHE, can be met through telecommunications means. Below we will discuss this impact on teaching physicians, but here let’s make this applicable to incident-to services. Services rendered by QHP individuals (nurse practitioner, physician assistant, clinical nurse midwife, clinical psychologist, or LCSW) can only meet incident-to rule specifications if the supervising MD is in telecommunications with the QHP at the time of the encounter. While this is possible, it seems unlikely that two providers would be involved in a telehealth encounter. However, if this occurs, then incident-to is met.
The IFR states that direct supervision, during the PHE, can be met through telecommunications means. Below we will discuss this impact on teaching physicians, but here let’s make this applicable to incident-to services. Services rendered by QHP individuals (nurse practitioner, physician assistant, clinical nurse midwife, clinical psychologist, or LCSW) can only meet incident-to rule specifications if the supervising MD is in telecommunications with the QHP at the time of the encounter. While this is possible, it seems unlikely that two providers would be involved in a telehealth encounter. However, if this occurs, then incident-to is met.
Teaching physician services (page 106 - 108)
The question quickly emerged about teaching physician services and if residents can provide telehealth encounters. The answer is a resounding yes, as made guidance through the IFR, provided preceptorship with direct supervision is met. As stated above, direct supervision throughout the PHE can be met through telecommunications applications that include real-time audio and video. Direct supervision through these specifications applies to services rendered in primary care exception areas, non-primary care exception areas, and also in reading test and imaging results.
The question quickly emerged about teaching physician services and if residents can provide telehealth encounters. The answer is a resounding yes, as made guidance through the IFR, provided preceptorship with direct supervision is met. As stated above, direct supervision throughout the PHE can be met through telecommunications applications that include real-time audio and video. Direct supervision through these specifications applies to services rendered in primary care exception areas, non-primary care exception areas, and also in reading test and imaging results.
The IFR includes many other rules and regulations that are applicable during this PHE, but these are the more pressing matters related to coding, billing, and documentation. Other services can be provided through telehealth means, such as ED visits, mental health services, and other therapy services. This article has focused on office/clinic visit services.
I mentioned at the beginning of this article a concern made by a nurse practitioner friend of mine, fearing lay off from the family practice that she currently works for. I bring this into the conversation of this article because with these CMS relaxations, which are also being followed by most commercial carriers, treating patients through telehealth encounters (upon consent by the patient) is not only a way to continue patient care and interaction, but also to keep clinical teams productive and billings consistent. Organizations are allowed to educate their patients on telehealth services in lieu of cancelling appointments. Upon verbal consent, the patient encounter can proceed as a telehealth service.
Daily, whether treatment related or geographical exposure, COVID-19 details are changing. Upon writing this article today, national news is advising that our current PHE could linger until the beginning of June. Daily, we are being introduced to a new interim normal. Dedicate an individual on your team to begin a patient education initiative on telehealth services. Be creative, create a video for your website (everyone has a video camera on their phone), send out postcards, make patient calls, or reference CMS patient deliverables on how they can maintain chronic issues, treat acute complaints, and maintain their wellness in the safety of their quarantined home.
NAMAS has created a resource page with a wide variety of COVID-19 support. We are committed to updating this webpage and providing newsworthy blasts of information to all of our contacts. Please visit this site at https://namas.co/covid-19-support/.
Also, CMS published a wonderful video (approximately 16 minutes in length) outlining many of the details of telehealth services during the COVID-19 crisis. This video can be found at: https://www.youtube.com/watch?v=bdb9NKtybzo&feature=youtu.be
Shannon DeConda, CPC, CPC-1, CPMA, CEMC, CMSCS, is the Founder and President of the National Alliance of Medical Auditing Specialists (NAMAS) as well as the President of Coding & Billing Services and a Partner at DoctorsManagement, LLC.
Ms. DeConda has over 16 years of experience as a multi-specialty auditor and coder. She has helped coders, medical chart auditors, and medical practices optimize business processes and maximize reimbursement by identifying lost revenue. www.namas.co